![]()
Updated Nov-2025 Pass AB-Abdomen Exam - Real Practice Test Questions
Download Free ARDMS AB-Abdomen Real Exam Questions
NEW QUESTION # 12
Which sonographic appearance of the normal epididymis is the most common?
- A. Isoechoic to the testis
- B. Anechoic with hyperechoic borders
- C. Hypoechoic with irregular borders
- D. Homogeneous compared to the testis
Answer: D
Explanation:
The normal epididymis typically appears as a homogeneous structure that is either isoechoic or slightly hypoechoic compared to the testis. The most accurate description is "homogeneous compared to the testis," meaning the texture is uniform. It is not anechoic, nor does it typically show irregular borders unless pathology is present.
According to Rumack's Diagnostic Ultrasound:
"The normal epididymis appears homogeneous and is isoechoic or slightly hypoechoic relative to the testis." (Rumack CM et al., Diagnostic Ultrasound, 5th ed.) Reference:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier; 2017.
AIUM Practice Parameter for Scrotal Ultrasound, 2020.
-
NEW QUESTION # 13
Which condition is demonstrated in this image?
- A. Hydronephrosis
- B. Intussusception
- C. Pyloric stenosis
- D. Gastritis
Answer: C
Explanation:
The ultrasound image clearly demonstrates a thickened and elongated pyloric muscle with a visible channel, which is characteristic of hypertrophic pyloric stenosis (HPS). This condition is most commonly seen in male infants between 2 and 8 weeks of age who present with non-bilious projectile vomiting, dehydration, and a palpable "olive-like" mass in the right upper quadrant.
Ultrasound is the imaging modality of choice and is highly sensitive and specific for diagnosing pyloric stenosis.
Key sonographic criteria for HPS:
* Muscle thickness >3 mm
* Pyloric channel length >15-17 mm
* "Target sign" or "doughnut sign" on transverse imaging (concentric rings)
* "Cervix" or "railroad track sign" on longitudinal imaging (elongated canal with echogenic center) Differentiation from other options:
* A. Intussusception: Also shows a target sign, but it occurs in the right lower quadrant or periumbilical region, not in the gastric antrum.
* C. Hydronephrosis: Refers to dilation of the renal pelvis and calyces - not gastrointestinal.
* D. Gastritis: May show gastric wall thickening but lacks the distinct elongated, thickened pyloric muscle seen here.
References:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018.
Chapter: Gastrointestinal Tract, pp. 474-479.
American College of Radiology (ACR) Appropriateness Criteria - Vomiting in Infants Up to 3 Months of Age.
AIUM Practice Parameter for the Performance of a Pediatric Abdominal Ultrasound Examination, 2020.
NEW QUESTION # 14
Which scanning technique is most beneficial when imaging the appendix?
- A. Apply graded compression around the patient's area of pain
- B. Apply light pressure around the patient's area of pain
- C. Image small bowel transversely to evaluate for peristalsis
- D. Image in the longitudinal plane around the iliac vessels
Answer: A
Explanation:
Graded compression technique is the gold standard for ultrasound evaluation of the appendix. It displaces gas and compresses overlying bowel loops to visualize the noncompressible, blind-ending tubular appendix directly at the point of maximal tenderness.
According to Rumack's Diagnostic Ultrasound:
"Graded compression using steady, increasing pressure displaces gas and bowel to optimize visualization of the appendix." Reference:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
AIUM Practice Parameter for the Performance of an Ultrasound Examination of the Abdomen, 2020.
-
NEW QUESTION # 15
Which condition is associated with multiple pancreatic cysts?
- A. Cystic fibrosis
- B. Autosomal recessive polycystic kidney disease
- C. Beckwith Wiedemann syndrome
- D. Von Hippel Lindau syndrome
Answer: D
Explanation:
Von Hippel-Lindau (VHL) syndrome is a genetic disorder associated with multiple pancreatic cysts, pancreatic neuroendocrine tumors, and other systemic neoplasms. While cystic fibrosis can produce thickened pancreatic secretions, it rarely causes true pancreatic cysts.
According to Rumack's Diagnostic Ultrasound:
"Multiple pancreatic cysts are strongly associated with Von Hippel Lindau syndrome." Reference:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
WHO Classification of Digestive System Tumors, 5th ed., IARC, 2019.
-
NEW QUESTION # 16
Which technique may provide better visualization of the common bile duct in a patient with hepatic steatosis?
- A. Scan patient after a fatty meal
- B. Increase dynamic range
- C. Decrease transducer frequency
- D. Decrease overall gain
Answer: C
Explanation:
In hepatic steatosis (fatty liver), increased echogenicity can obscure visualization of deeper structures like the common bile duct. Lowering the transducer frequency increases sound wave penetration, allowing better visualization of deep structures despite increased liver echogenicity. Decreasing gain or increasing dynamic range primarily adjusts image brightness and contrast but does not improve penetration.
According to Rumack's Diagnostic Ultrasound:
"Lower frequency transducers are used to improve penetration and visualization of deeper structures in patients with fatty liver." Reference:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
AIUM Practice Parameter for the Performance of Abdominal Ultrasound Examinations, 2020.
-
NEW QUESTION # 17
Which imaging technique best demonstrates ureteral patency?
- A. Graded compression
- B. Color Doppler
- C. Gray scale
- D. Spectral Doppler
Answer: B
Explanation:
Color Doppler imaging can detect ureteral jets, which represent urine entering the bladder from the ureters.
The presence of bilateral ureteral jets confirms ureteral patency. Gray scale may show hydronephrosis but does not directly assess flow.
According to Rumack's Diagnostic Ultrasound:
"Color Doppler demonstrates ureteral jets within the bladder, confirming ureteral patency." Reference:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
AIUM Practice Parameter for Renal Ultrasound, 2020.
-
NEW QUESTION # 18
Which vessel is indicated by the arrow on this image?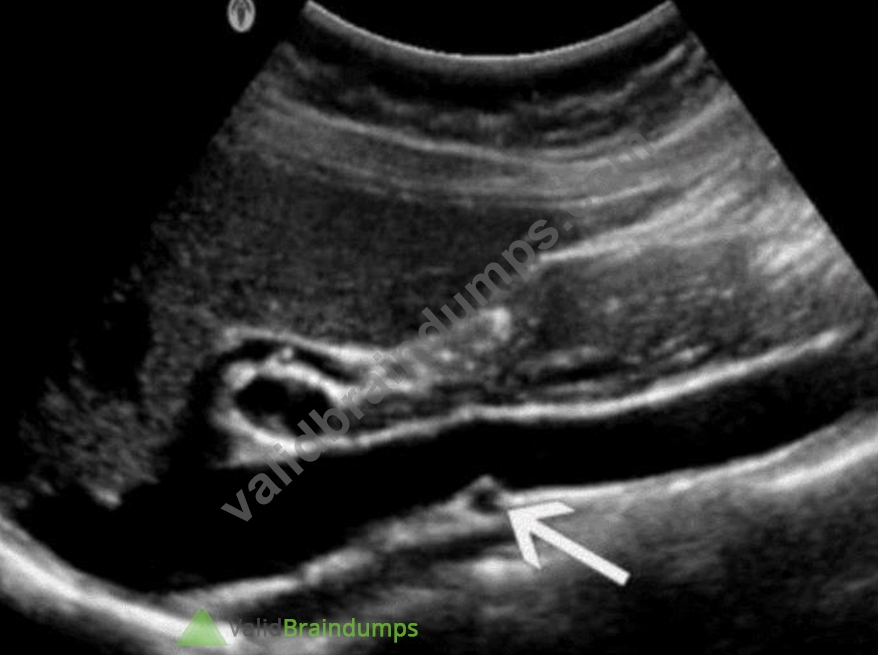
- A. Left renal vein
- B. Proper hepatic artery
- C. Superior mesenteric artery
- D. Right renal artery
Answer: C
Explanation:
The ultrasound image demonstrates a transverse view of the abdominal vasculature, where the arrow is pointing to a circular vascular structure anterior to the aorta and posterior to the body of the pancreas - consistent with the superior mesenteric artery (SMA).
The SMA originates from the anterior aspect of the abdominal aorta just below the level of the celiac trunk and courses anterior to the left renal vein and uncinate process of the pancreas. On transverse ultrasound, it is often seen in cross-section as a round, pulsatile structure with echogenic walls, situated just anterior to the aorta. This appearance is known as the "target sign" or "bull's-eye" appearance.
Vessel Position Landmarks (transverse plane):
* Aorta: Posterior and central
* SMA: Just anterior to the aorta
* Left renal vein: Passes between the aorta and SMA (nutcracker location)
* Right renal artery: Courses posterior to the IVC toward the right kidney Differentiation from other options:
* A. Proper hepatic artery: Typically visualized within the liver hilum (portal triad), not in this anatomic location.
* C. Left renal vein: Seen in transverse as a longer, oval structure crossing anterior to the aorta and posterior to the SMA.
* D. Right renal artery: Arises laterally from the aorta and courses posterior to the IVC - not visualized in this axial midline location.
References:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018.
Chapter: Vascular Anatomy and Abdominal Vessels, pp. 471-475.
American Institute of Ultrasound in Medicine (AIUM) Practice Parameter for the Performance of an Ultrasound Examination of the Abdomen and/or Retroperitoneum, 2020.
Radiopaedia.org. Superior mesenteric artery: https://radiopaedia.org/articles/superior-mesenteric-artery
-
NEW QUESTION # 19
Where is the main pancreatic duct located?
- A. Dorsal to the superior mesenteric artery
- B. Ventral to the pancreatic body
- C. Dorsal to the common bile duct
- D. Medial to the superior mesenteric vein
Answer: D
Explanation:
The main pancreatic duct (duct of Wirsung) runs through the central portion of the pancreas, medial and slightly posterior to the superior mesenteric vein (SMV). It converges with the common bile duct near the ampulla of Vater.
According to Moore's Clinically Oriented Anatomy:
"The main pancreatic duct runs centrally within the gland and lies medial to the superior mesenteric vein." Reference:
Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 8th ed. Wolters Kluwer, 2018.
Gray's Anatomy for Students, 4th ed., Elsevier, 2019.
-
NEW QUESTION # 20
Which arteries are the immediate branches of the celiac trunk?
- A. Proper hepatic, splenic, and gastroduodenal
- B. Common hepatic, splenic, and right gastric
- C. Proper hepatic, splenic, and supraduodenal
- D. Common hepatic, splenic, and left gastric
Answer: D
Explanation:
The celiac trunk arises from the abdominal aorta and immediately divides into three primary branches:
* Left gastric artery
* Common hepatic artery
* Splenic artery
The proper hepatic and gastroduodenal arteries are secondary branches of the common hepatic artery.
According to Moore's Clinically Oriented Anatomy:
"The celiac trunk trifurcates into the left gastric, common hepatic, and splenic arteries." Reference:
Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 8th ed. Wolters Kluwer, 2018.
Gray's Anatomy for Students, 4th ed., Elsevier, 2019.
NEW QUESTION # 21
Which outcome would be present if the sample volume gate is larger than the examined vessel?
- A. Aliasing
- B. Indeterminate flow direction
- C. Spike turbulence
- D. Spectral noise
Answer: D
Explanation:
When the sample volume (gate) is too large, it captures signals from both the vessel and surrounding tissues or adjacent flows. This leads to a broadening of the spectral waveform and produces "spectral noise" or
"spectral broadening," reducing the accuracy of velocity measurements and waveform analysis. Aliasing results from high velocity relative to the Nyquist limit, not from gate size.
According to Zwiebel's Introduction to Vascular Ultrasound:
"Increasing the sample volume beyond the vessel size causes spectral broadening, resulting in spectral noise and inaccurate Doppler measurements." Reference:
Zwiebel WJ, Pellerito JS. Introduction to Vascular Ultrasound. 6th ed. Elsevier, 2019.
AIUM Practice Parameter for Spectral Doppler Ultrasound, 2021.
-
NEW QUESTION # 22
What is the most common malignancy of the prostate?
- A. Sarcoma
- B. Seminoma
- C. Hamartoma
- D. Adenocarcinoma
Answer: D
Explanation:
Prostate adenocarcinoma is by far the most common malignancy of the prostate gland, typically arising in the peripheral zone. Seminoma is a testicular tumor, sarcomas are rare in the prostate, and hamartomas are benign lesions.
According to Rumack's Diagnostic Ultrasound:
"Adenocarcinoma accounts for the vast majority of prostate cancers and is typically located in the peripheral zone." Reference:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
AIUM Practice Parameter for Prostate Ultrasound, 2020.
-
-
NEW QUESTION # 23
Which abnormality is depicted in this image of a patient who presents with a fever following a liver biopsy?
- A. Cyst
- B. Biloma
- C. Abscess
- D. Hematoma
Answer: C
Explanation:
The sonographic image shows a complex fluid collection within the liver parenchyma, with internal echoes and possibly septations, consistent with an abscess. In the clinical context of post-procedural fever following a liver biopsy, a liver abscess is the most likely diagnosis.
A liver abscess appears on ultrasound as a hypoechoic or complex fluid collection that may contain internal debris, septations, or gas (which may produce reverberation artifacts). These features distinguish it from other post-procedural complications.
* A cyst (Option A) typically appears as an anechoic, well-defined lesion with posterior acoustic enhancement and no internal debris-this does not match the image or clinical setting.
* A biloma (Option B) is a bile collection that can appear similar to a cyst or fluid collection but typically occurs due to bile leak; however, fever and internal complexity on ultrasound more strongly suggest abscess.
* A hematoma (Option D) may also appear complex but usually presents with pain and not fever unless secondarily infected. Over time, hematomas evolve in appearance but lack septations and gas unless superinfected.
Reference:
Rumack, Carol M., et al. Diagnostic Ultrasound.5th ed., Elsevier, 2018. Chapter: Hepatobiliary System, pp.
107-111.
American Institute of Ultrasound in Medicine (AIUM) Practice Parameter for the Performance of an Ultrasound Examination of the Abdomen and/or Retroperitoneum.
NEW QUESTION # 24
Which type of artifact is indicated by the arrows on this image?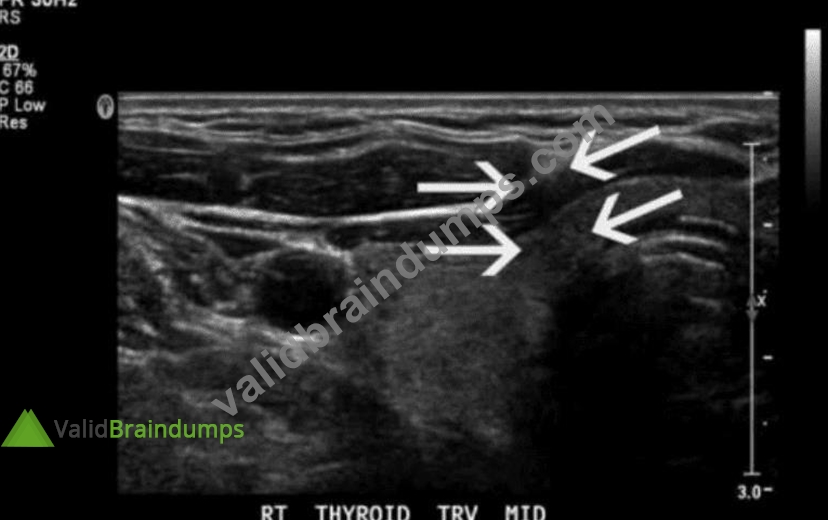
- A. Edge shadow
- B. Speed error
- C. Comet tail
- D. Focal enhancement
Answer: A
Explanation:
The ultrasound image of the thyroid clearly shows posterior shadowing originating from the lateral edges of a rounded structure, which is indicative of edge shadow artifact. Edge shadowing occurs when an ultrasound beam passes tangentially to a rounded or curved structure, such as a cyst or blood vessel. The difference in sound wave refraction and beam divergence at the edges leads to decreased echo signals deep to the edges, creating linear hypoechoic bands - which is exactly what the arrows are pointing to in the image.
Edge shadow artifact is purely a result of beam physics and not a real anatomic or pathologic finding.
Key characteristics of edge shadowing:
* Appears as a narrow, linear hypoechoic (dark) shadow extending deep to the edge of a curved interface (e.g., cyst, vessel, thyroid nodule)
* Caused by refraction and beam deflection, leading to reduced beam intensity distal to the edges
* Most commonly seen adjacent to cysts or fluid-filled structures
Differentiation from other options:
* A. Focal enhancement: Appears as increased echogenicity distal to a fluid-filled structure due to lower attenuation of the sound beam through fluid (opposite of shadowing).
* C. Speed error: A less common artifact that results in displacement of structures due to variation in assumed sound speed.
* D. Comet tail: A reverberation artifact that appears as a series of closely spaced bright echoes, often associated with metallic objects or cholesterol crystals in adenomyomatosis.
References:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018.
Chapter: Ultrasound Physics and Artifacts, pp. 38-42.
Kremkau FW. Sonography Principles and Instruments. 9th Edition. Elsevier, 2015. Chapter: Image Artifacts, pp. 132-136.
NEW QUESTION # 25
Which structure is most likely shown in this image of the right lower quadrant?
- A. Appendix
- B. Fallopian tube
- C. Ureter
- D. Jejunum
Answer: A
Explanation:
The ultrasound image shows a blind-ending, non-compressible, tubular structure in the right lower quadrant with a target or bullseye appearance in transverse section - highly suggestive of the appendix.
Sonographic features of the appendix (especially in suspected appendicitis):
* Blind-ending tubular structure arising from the cecum
* Non-compressible on graded compression
* Diameter >6 mm is suggestive of appendicitis
* May demonstrate a "target sign" in transverse view (concentric ring-like appearance)
* Increased echogenicity of surrounding fat in cases of inflammation
* May contain an appendicolith or show hyperemia on color Doppler if inflamed The location (right lower quadrant) and appearance in this case are classic for the normal or potentially inflamed appendix.
Differentiation from other options:
* A. Fallopian tube: Located more in the adnexal regions and usually not visible unless distended (e.g., hydrosalpinx).
* B. Ureter: Usually not visualized on ultrasound unless dilated due to obstruction.
* D. Jejunum: Has valvulae conniventes ("keyboard sign") and peristalsis; does not present with a blind- ending tubular appearance from the cecum.
References:
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018.
Chapter: Gastrointestinal Tract, pp. 460-468.
American College of Radiology (ACR). ACR Appropriateness Criteria - Right Lower Quadrant Pain - Suspected Appendicitis.
AIUM Practice Parameter for the Performance of a Pediatric Abdominal and/or Retroperitoneal Ultrasound Examination, 2020.
NEW QUESTION # 26
Which structures are located within the testes?
- A. Seminiferous tubules
- B. Aberrant ductules
- C. Gubernacula
- D. Efferent ductules
Answer: A
Explanation:
The seminiferous tubules are coiled structures located within the testes where spermatogenesis (sperm production) occurs. They are surrounded by Sertoli and Leydig cells that support spermatogenesis and testosterone production.
* Gubernacula (A) are fetal structures involved in testicular descent.
* Efferent ductules (B) connect the rete testis to the epididymis but are not located within the testicular parenchyma.
* Aberrant ductules (C) are accessory ducts found outside the testis.
Reference Extracts:
* Moore KL, Dalley AF, Agur AM. Clinically Oriented Anatomy. 7th ed. Lippincott Williams & Wilkins, 2013.
* Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
NEW QUESTION # 27
Which vascular condition is most consistent with patent cutaneous para-umbilical channels and portal hypertension?
- A. Esophageal varices
- B. Caput medusae
- C. Splenic vein varices
- D. Coronary vein varices
Answer: B
Explanation:
Caput medusae refers to dilated paraumbilical veins due to portal hypertension. When portal venous pressure rises, collateral channels may open along the ligamentum teres and recanalized paraumbilical vein, resulting in visible dilated veins radiating from the umbilicus.
* Esophageal varices (B) are gastroesophageal collaterals.
* Coronary vein varices (C) involve gastric veins.
* Splenic vein varices (D) are typically localized to the splenic hilum.
Reference Extracts:
* Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier, 2017.
* Gore RM, Levine MS. Textbook of Gastrointestinal Radiology. 4th ed. Saunders, 2015.
-
NEW QUESTION # 28
......
AB-Abdomen Dumps 100 Pass Guarantee With Latest Demo: https://www.validbraindumps.com/AB-Abdomen-exam-prep.html
Pass Your Exam With 100% Verified AB-Abdomen Exam Questions: https://drive.google.com/open?id=1Jhe5LxOEcOt7-zoM4O3VV4rUzPGVCiWG